Credit: Artist unknown.
Wikipedia has an excellent, detailed article about dysfunctional family dynamics. Here I am just going to talk about the roles various family members play, and the kinds of families that become dysfunctional. If you’d like to read the whole article, click on this link:
https://en.wikipedia.org/wiki/Dysfunctional_family
Dysfunctional families are usually of two types:
1. One or more of the parents are active alcoholics or addicted to drugs.
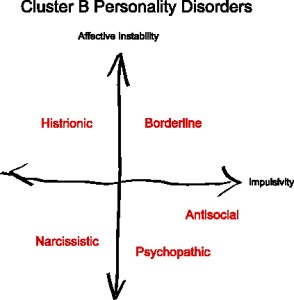
2. One or more of the parents have a Cluster B disorder, usually Narcissistic Personality Disorder but sometimes Borderline Personality Disorder, Antisocial Personality Disorder, or Histrionic Personality Disorder (or a combination of any of these).
The Cluster B Connection.
Outside of alcoholics and drug addicts, dysfunctional family dynamics are most prevalent when one or both of the partners suffer from a Cluster B disorder, especially Narcissistic Personality Disorder or Malignant Narcissism. After NPD, BPD is the most common disorder seen in the head of a dysfunctional family, though because it’s more common in women and Borderlines have more empathy than narcissists, BPD is most often seen in the codependent, passive partner.
ASPD (psychopathy or sociopathy) rarely appears by itself in dysfunctional families, as antisocial people and psychopaths tend to not be raising children at all (either because they’re incarcerated, their children have already been removed from the home, or they simply have no interest in raising children,) but a parent could have Malignant Narcissism, which is a combination of NPD and ASPD. Also, people with pure ASPD, though more likely to be criminals or involved in illegal activities, tend to be less emotionally abusive than people with NPD or even BPD. They are merely selfish and lack empathy, and they are manipulative to get what they want, but they don’t care about getting emotional supply from others so they don’t engage in mind games like gaslighting, triangulating, projecting, and scapegoating (unless there is a material reward involved or they are trying to avoid culpability). However, some people with ASPD are sadistic and enjoy tormenting family members for fun.
Of all the Cluster B disorders, HPD is probably the least toxic (Histrionics are shallow, attention seeking, and dramatic, but not usually that abusive), but HPD is usually comorbid with another Cluster B disorder, such as NPD.
In some cases, a non-Cluster B mental illness (such as Bipolar disorder) that causes abusive acting-out behavior may be the culprit, but it’s less common because most other mental disorders are less easily hidden from others and the person appears “crazier.” Non-Cluster B disorders are also more easily treated with drugs or therapy, and except for psychotic disorders such as Schizophrenia, the afflicted person knows they have a problem and are more likely to seek help.
Cluster B and addictive disorders.
Parents of dysfunctional families can also be both mentally ill and addicted to drugs or alcohol. The two often go together. In fact, alcoholism and drug addiction are extremely common in people with Cluster B disorders. Alcohol and drugs are their attempt to fill the emptiness they feel inside themselves.
Even if an alcoholic or drug addict doesn’t have an underlying Cluster B disorder, the behavior of an active addict/alcoholic is very similar to someone who has NPD. The only difference in the behavior of a narcissist and someone with active alcoholism is that for the narcissist, the “fix” is emotional; for the alcoholic, it’s chemical. A non-Cluster B active addict or alcoholic can be every bit as emotionally abusive, self-centered, and manipulative as someone with NPD. Only getting their next fix is important. (As an aside, it’s interesting to me that the 12 steps of AA and other 12-step programs almost all address the problem of narcissism by encouraging humility, responsibility, and amend-making. A person on a so-called “dry drunk” is basically a sober person acting out in narcissistic ways, which may be their nature).
The Codependent Partner.
Sometimes only one partner has a mental disorder or addiction, but the non-afflicted parent is always going to be codependent to them. The codependent parent, whether they have a disorder or not, almost always suffers from PTSD or Complex PTSD. If both parents have a Cluster B disorder (which I think is usually the case), the one who has NPD or Malignant Narcissism is almost always going to call all the shots and dominate the other family members. If a Borderline is paired up with a Narcissist, the Borderline is almost always going to be codependent to the Narcissist, colluding in the abuse but also being abused themselves. Similarly, if a Covert Narcissist is paired up with an Overt Narcissist, the Covert one is going to be codependent to them and possibly abused. Such a scenario can lead to the Borderline or Covert Narcissist developing Stockholm Syndrome (identifying with and colluding with their abuser). Non-Cluster B codependents can also develop Stockholm Syndrome, because it’s a complication of C-PTSD. The codependent parent often (but not always) has a high degree of empathy, which is what drew them to the narcissist in the first place, in a misguided belief that they could “fix” them or they were led to believe that the narcissist could “rescue” them.
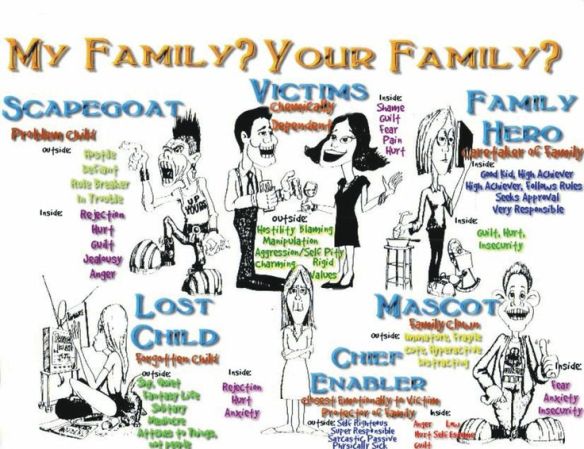
The Roles of the Children.
In the ACON community, there’s a lot of talk about Scapegoats and Golden Children, but there are other roles children can play in a family that are rarely addressed. In a two child family, most likely there will be a scapegoat and a golden child, but in larger families, there can also be a Lost Child, a Clown, and a Rescuer (codependent). It’s unhealthy for a child to be in any of these roles, but the Scapegoat and Golden Child role are probably the most dangerous to a child’s mental and emotional health, for different reasons. Even in a two-child family, the roles can shift back and forth (according to the Wikipedia article, families in which the children’s roles change and shift are called Balkanized families–this alludes to the constantly shifting loyalties and borders of the Balkan countries in Eastern Europe).
1. The Scapegoat.
Both this and the Golden Child role are the soul-killing roles, but for different reasons. The Scapegoat is the child who is targeted by the narcissistic (or alcoholic) parent. The parent often is able to get the rest of the family to serve as flying monkeys and gang up on that child, projecting anything they don’t want to “own” onto them. Like the sacrificial goats described in the Bible who were banished to the wilderness and tormented by villagers, the Scapegoated child carries all the shame the rest of the family doesn’t want to confront or deal with. All the unwanted emotions and bad qualities are unloaded and projected onto them, so the abusers don’t have to confront or deal with these problems in themselves.
Usually it’s the most sensitive child of the family who becomes the Scapegoat, because that child tends to be the Truth Teller, the only family member who can see the dysfunction and may even react against it. The most sensitive child, being the child who shows the most emotion, is also a threat to the narcissists in the family because emotional expression is such a frightening thing to them. In many, if not most dysfunctional families, the expression of emotion is not allowed. So the most emotional or sensitive child becomes the scapegoat, especially if they rebel against the dysfunction or criticize it.
The Scapegoat may be assigned the role of Bad Child, the Loser, the Stupid One, the Ugly One, the Crazy One, the Weak One, or any combination of these. No matter what they do, they cannot please the parents (or the siblings who have been turned against them). Scapegoat Children usually develop severe C-PTSD or possibly another mental disorder, and having been trained to be victims and never given the emotional, financial or other tools to succeed in life, tend to fulfill their families’ predictions of being “losers,” so then their families can say to others, “See? This child really is worthless.”
Scapegoated children also tend to attract other abusers throughout their lives and are at risk for being targeted for bullying even as adults and for entering into abusive relationships. If the adult child doesn’t go No Contact, the abuse continues, usually through some form of isolation, silent treatment, or exclusion. Scapegoated adults are talked badly about by the family and not invited to family functions. They are given no emotional or financial support, even though other members of the family are given these things. It’s not unusual for a scapegoated adult child to be living in poverty, even if their families are wealthy–not only because they were denied financial support when they needed it, but also because their self esteem took such a terrible beating that they have no confidence at all and never take any risks that could improve their lives. Severe C-PTSD can also cause a person to have an inability to focus or concentrate or set realistic goals.
A Scapegoat isn’t always a child. It can also be a parent, in which the children are turned against that parent by the abusive one.
2. The Golden Child.

The Golden Child, often (but not always) the eldest child, is the parent’s trophy, pride and joy. The parents may seem to love that child, but being incapable of real love, their “love” is conditional and is based on their fantasy of what they want that child to be, not on who the child really is. The child is assigned to be a Mini Me of the narcissistic parent.
The Golden Child, basking in constant approval, showered with toys and gifts, never held accountable for any wrongdoing (which may be projected onto the Scapegoat), and often recruited as a co-abuser in the abuse of the Scapegoat, grows up entitled, grandiose, and spoiled. Because their Real Self has never been appropriately mirrored and their less than perfect traits are ignored or projected onto someone else, and because they were rewarded for playing a the role of the Perfect One, a Golden Child in a family is the most likely to develop NPD and become a clone of the abusive parent. In this way their souls are destroyed even more than the Scapegoat’s. To continue to be the parent’s favorite, they had to play a role which became internalized. This becomes their False Self. After awhile, they are no longer able to access their Real Self at all. Golden Children who have become narcissistic continue their entitled, bullying, manipulative, grandiose behavior into adulthood and are likely to head dysfunctional families themselves, continuing the cycle.
A non-Golden Child, even a Scapegoat, can become a narcissist too (usually the covert form of NPD), for self-protection, but Golden Children tend to develop the grandiose, malignant form of narcissism and as such, are the least likely to ever seek help for their disorder or admit they have become abusers themselves.
3. The Lost Child.

In larger families (three or more children), one child is likely to be ignored and treated as if they don’t exist. This isn’t a form of silent treatment; it’s as if the parents don’t notice the child is there at all. The Lost Child isn’t victimized like the Scapegoat, but they aren’t spoiled either. They may or may not be recruited to assist in the abuse of the Scapegoat, but they won’t necessarily be punished if they don’t cooperate; they will simply be ignored. The Lost Child tends to be quiet and shy, and not make any waves. They are probably aware of the family dysfunction and may sympathize with the scapegoat (but don’t let anyone know this). As they grow older, they may crave attention or develop addictions, or they may remain shy and retiring throughout their lives. They tend to avoid confrontation and drama, and may become extremely introverted.
4. The Clown/Mascot.

The Clown/Mascot attempts to divert attention away from the family dysfunction (and also get attention for themselves) by making light of everything. Everything becomes a joke to them, and they even use their own families as sources for humor. Clowns can be disruptive in class as children, to get attention, but because of their ability to see the humor in things, they tend to be outgoing and develop a large circle of friends during adolescence and adulthood (even if they are never taken very seriously). Family Mascots are almost never scapegoated, because they entertain everyone and take the focus off the family problems.
David Sedaris, a writer and humorist, is a good example of this dynamic at play. Several writers in the ACON community (and even outside that community) were outraged by Sedaris’ callous essay (“Now We Are Five,” which appeared in the New Yorker after his younger sister, Tiffany, committed suicide). Tiffany was clearly the family scapegoat and had evidently gone No Contact with the rest of the family. At the time of her death, she was living in poverty and only had, as her father put it, “two lousy boxes” of belongings. I don’t know all the details, but it seems as if she was offered no support, either emotionally or financially, in spite of the family’s wealth and Sedaris’ success as a writer. She was probably mentally ill, but her mental illness may have been due to being the family reject.
In a candid interview Sedaris gave for Vice, he describes Tiffany and her relationship with the rest of the family. His words are very telling.
Even as a child I looked at my sister and wondered what that would be like, not to feel the warmth of my mother’s love. Tiffany didn’t. There was always a nervous quality about her, a tentativeness, a desperate urge to be in your good graces. While the rest of us had eyes in the front of our heads, she had eyes on the sides, like a rabbit or a deer, like prey, always on the lookout for danger. Even when there wasn’t any danger. You’d see her trembling and think, You want danger? I’ll give you some danger…
It’s been suggested that David Sedaris is himself a narcissist (possibly the golden child) and that could certainly be true, but I also suspect he served a secondary role as the family Clown/Mascot. His callousness toward Tiffany in his famous essay (and grandiosity about how great the rest of the Sedaris family was–it’s very common for narcissists who were golden children to hold their dysfunctional families up as paragons of perfection) seemed to be drawn both from narcissism and from a need to hide his anger and pain behind a wall of humor. Here’s a link to his essay (it’s heartbreaking and may be triggering):
Now We Are Five
The accompanying photo is interesting. Tiffany, the second to youngest child in a family of six children, sits in the bottom right hand corner. Her hair is cut short and unkempt, and she looks very unhappy. David, wearing the glasses, stands above her. Actually, none of the kids look very happy. Not a smile in the bunch. Something’s definitely not right about this family. It’s common to see family portraits where no one is smiling in the 18th or 19th centuries, but not in the late 1960s, when this photo was taken. Here’s another photo, from the Vice interview, where only Tiffany (again in the bottom right hand spot) looks desperately unhappy and disconnected from her siblings.
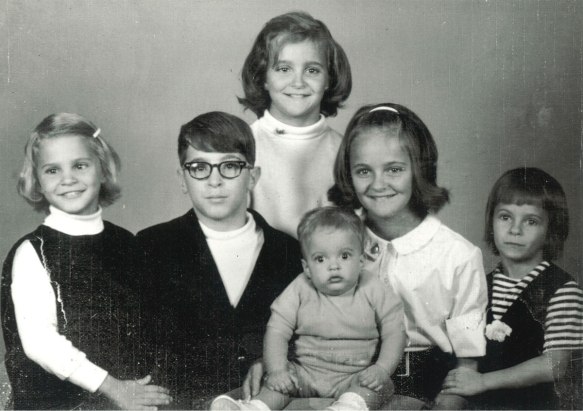
Credit: Vice.com / Left to right: Amy, David, Gretchen, Paul, Lisa, and Tiffany
I used to enjoy Sedaris’ writings and looked forward to his books and essays, but after this essay, I just can’t read him anymore. (Augusten Burroughs is a better alternative and doesn’t seem to be a narcissist).
In spite of their raucous and jovial manner, Clowns are likely to be depressed because they have never learned to confront or deal with their true feelings. They hide behind a wall of laughter. Their sense of humor is really just a cover for their pain. Many Clowns become addicted to drugs or alcohol, and a few become suicidal. Many of our great comedians served the Clown role in their families. I don’t think it’s a coincidence that so many of them had drug issues or killed themselves.
5. The Rescuer.
This is the codependent child who attempts to “fix” the family dysfunction by being obedient, always good, non-confrontational, overly generous, and self-sacrificing. The Rescuer may be highly empathic. The Rescuer tries to serve all the needs of the narcissistic/addicted parent, which of course is not possible. They will never argue with or criticize the narcissistic parent, and are always trying to get everyone to get along, which also is not possible. They may be the only family member who doesn’t abuse the Scapegoat, but they might if they feel like it’s required. However, even if they do collude in the Scapegoat’s abuse, they will be less abusive than the other family members, tending to take a back seat or even sympathize with the Scapegoat in private. In trying to please everyone, they please no one, and grow up feeling impotent and helpless. It’s a no-win situation.
When Rescuers become adults, they tend to unconsciously look for other abusers to “rescue,” having failed to do so in their families of origin. Like Scapegoats, Rescuers are likely to become abused themselves as adults, but it’s hard for them to leave an abuser because of their high level of empathy which keeps them tied to the abuser in their attempt to want to “help” them. They also tend to fall for an abuser’s promises to change and are easily “hoovered” back into a codependent relationship.
Shifting Roles.
In Balkanized families, the child roles can shift. The most common situation is a Golden Child becoming a Scapegoat, often upon reaching adulthood, if they fail to fulfill the unrealistic expectations put on them. (“You were such a disappointment to me!”) If a Scapegoat goes No Contact or leaves the family for some other reason, another child, possibly the Lost Child, becomes the new Scapegoat. Someone has to carry all the family shame. If the family only has two children, the Golden Child may find themselves suddenly scapegoated or serving both roles.
Children who serve as both Scapegoats and Golden Children (very common in only children) often develop Borderline Personality Disorder as well as severe C-PTSD and possibly other mental disorders like Dissociative Identity Disorder (almost always the result of severe emotional abuse).
Serving as both a Scapegoat and Golden Child is the ultimate mindf*ck because there isn’t even any consistency. The child never knows if they will be punished or rewarded from one minute to the next. Their only advantage (if they are an only child) is that they don’t have siblings who have been turned into flying monkeys who collude in the abuse.
If the family ever develops a need for a new Scapegoat (if the Scapegoat goes No Contact, dies, or disappears), the Lost Child is usually picked as a replacement, due to their non-confrontational, malleable temperament and lack of any real pre-existing role in the family.