There seems to be a lot of misunderstanding about borderline personality disorder. I’ve noticed many people seem to confuse it with narcissistic personality disorder (NPD). While there ARE some overlapping symptoms (and it’s even been speculated by a number of mental health professionals that BPD is actually a less severe form of NPD), they are quite different from each other. I’d like to clear up a few of these misunderstandings and discuss both the similarities and the differences.
New DSM Criteria for BPD.
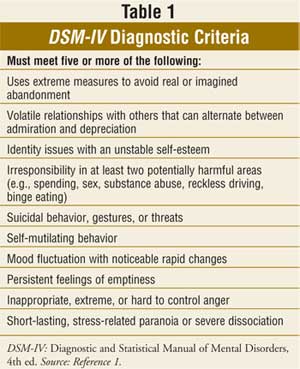
According the the DSM-V (2013), these are the diagnostic criteria for BPD (the new list of criteria is quite long and ponderous so I will not attempt to talk about each of these points here):
A. Significant impairments in personality functioning manifest by:
1. Impairments in self functioning (a or b):
a. Identity: Markedly impoverished, poorly developed, or unstable self-image, often associated with excessive self-criticism; chronic feelings of emptiness; dissociative states under stress.
b. Self-direction: Instability in goals, aspirations, values, or career plans.
AND
2. Impairments in interpersonal functioning (a or b):
a. Empathy: Compromised ability to recognize the feelings and needs of others associated with interpersonal hypersensitivity (i.e., prone to feel slighted or insulted); perceptions of others selectively biased toward negative attributes or vulnerabilities.
b. Intimacy: Intense, unstable, and conflicted close relationships, marked by mistrust, neediness, and anxious preoccupation with real or imagined abandonment; close relationships often viewed in extremes of idealization and devaluation and alternating between over involvement and withdrawal.
B. Pathological personality traits in the following domains:
1. Negative Affectivity, characterized by:
a. Emotional lability: Unstable emotional experiences and frequent mood changes; emotions that are easily aroused, intense, and/or out of proportion to events and circumstances.
b. Anxiousness: Intense feelings of nervousness, tenseness, or panic, often in reaction to interpersonal stresses; worry about the negative effects of past unpleasant experiences and future negative possibilities; feeling fearful, apprehensive, or threatened by uncertainty; fears of falling apart or losing control.
c. Separation insecurity: Fears of rejection by – and/or separation from – significant others, associated with fears of excessive dependency and complete loss of autonomy.
d. Depressivity: Frequent feelings of being down, miserable, and/or hopeless; difficulty recovering from such moods; pessimism about the future; pervasive shame; feeling of inferior self-worth; thoughts of suicide and suicidal behavior.
2. Disinhibition, characterized by:
a. Impulsivity: Acting on the spur of the moment in response to immediate stimuli; acting on a momentary basis without a plan or consideration of outcomes; difficulty establishing or following plans; a sense of urgency and self-harming behavior under emotional distress.
b. Risk taking: Engagement in dangerous, risky, and potentially self-damaging activities, unnecessarily and without regard to consequences; lack of concern for one’s limitations and denial of the reality of personal danger.
3. Antagonism, characterized by:
a. Hostility: Persistent or frequent angry feelings; anger or irritability in response to minor slights and insults.
C. The impairments in personality functioning and the individual’s personality trait expression are relatively stable across time and consistent across situations.
D. The impairments in personality functioning and the individual’s personality trait expression are not better understood as normative for the individual’s developmental stage or socio-cultural environment.
E. The impairments in personality functioning and the individual’s personality trait expression are not solely due to the direct physiological effects of a substance (e.g., a drug of abuse, medication) or a general medical condition (e.g., severe head trauma).
Is it really true that Borderlines can’t feel empathy?

BPD patient “Alice” (Kristen Wiig) in “Welcome to Me.”
The very first thing that stood out to me (and was not included in the older DSM criteria) is “lack of empathy.” Yes, it is a fact that many borderlines have difficulty feeling empathy under normal circumstances, but the reasons for this are vastly different than the lack of empathy seen in people with NPD.
Most people with BPD have the capacity to feel empathy, and can feel very guilty when they become aware (or it’s pointed out to them) that they have treated others badly, but because Borderlines have great difficulty regulating their emotional reactions and have an unfortunate tendency to lose themselves in their own drama when they perceive they are being attacked, at those times they can “forget” that others exist, and this can lead to them acting selfishly and disregarding the feelings of others. This can appear very narcissistic. It’s not that they CAN’T feel empathy though, because they certainly can. They can also feel remorseful. But it may take a disaster (such as losing a good friend or a broken relationship) for them to realize the damage their impulsive and selfish behavior has caused. If their bad behavior is pointed out to them by someone else–such as when the character Alice in the movie “Welcome to Me” loses her best friend Gina, who tells her how much she was hurt by Alice’s insults against her–they will feel remorse and try to make amends in whatever way they can.
Borderlines just want to be accepted.

Unlike narcissists, borderlines hate to be hated. Narcissists like any form of attention–negative or positive (and some even prefer to be hated!) while borderlines only want to be loved and thought of in a positive manner. Most of them WANT to be good people and WANT to be liked, but don’t always act in ways that make them seem very nice, due to their impulsivity and tendency to act out whatever emotions they are feeling at the moment.
Impulsivity is a primary issue with a borderline–a trait not shared by narcissists (but IS shared with people with ASPD)–because they fail to think ahead and consider consequences of their bad behavior.
Borderlines can act narcissistic because of their deep seated need to feel accepted. Most hate themselves (as do narcissists) and some can act grandiose and full of themselves in their attempts to be liked and admired. Deep inside, they feel worthless. It’s not hard to take down their braggadocio, however. Cut a borderline down to size and they may react with rage or tears (as will a narcissist) but are also more likely than a narcissist to admit you are right and they are really just worthless losers. They might even apologize profusely for acting so out of line.
I can’t help but think of the Wizard in The Wizard of Oz. An insecure little man who stood behind a curtain projecting the face of a raging tyrant onto a huge screen. When Toto pulled back the curtain to reveal who the “Wizard” really was, and Dorothy upbraided him for being a “very bad man,” the Wizard immediately became humble and apologized profusely to the group, telling them that yes, he was just a humbug. Some people have said the Wizard was a narcissist, but I think his behavior was more typical of a borderline. A narcissist would have continued to insist on his superiority, even with his true nature having been revealed–and his true nature would not have been so benign. The Wizard’s intentions for Dorothy and her friends were also good.
While a narcissist may rage and perhaps even use tears (to manipulate others into feeling sorry for them), they will almost never admit their wrongdoing or admit they are anything other than God’s gift to the world. Doing so is far too dangerous to them.
Why Borderlines act selfishly.

A borderline who is not under stress or in the midst of an emotional drama, or has learned to control their impulses through behavioral training like DBT–dialectical behavior training which was developed by Marsha Linehan (it does work–I can attest to its efficacy), can certainly feel empathy for others, and can be genuinely good and kind people. Genuine kindness and concern for others is rare in a narcissist and almost unheard of in a malignant narcissist. Borderlines generally have this capacity, but unfortunately, if they haven’t learned to control or regulate their emotions, their ability to feel for others or show a conscience is eclipsed by their own drama, which at the moment becomes all-important. They really just don’t know what they are doing, but if you call them out or make them suffer consequences, in most cases they will try to make it up to you.
Borderlines don’t live a lie.

Borderlines do not wear masks, as narcissists do. They cannot pretend to be someone they are not (or if try to, they usually fail miserably, like the wizard in The Wizard of Oz). They are not trying to fool you, even though to avoid rejection, they can be manipulative and use some of the same games (gaslighting, blame-shifting, rages, etc) that narcissists do. Borderlines, if anything, show TOO MUCH of themselves–and that includes the bad along with the good. With a borderline, it’s all WYSIWYG. They can’t wear a mask, because they lack the ability to plan things out ahead of time the way someone with NPD does. Wearing masks requires cunning and the ability to lie. While borderlines can and do lie (usually to exaggerate the pain they are facing or to idealize/devalue someone else), they can’t lie about who they are or what they’re feeling. In that sense, they’re even more honest than the average non-disordered person.
Idealization/devaluation in borderlines and narcissists.

Both narcissists and borderlines do tend to idealize and devalue other people, and both are guilty of black-or-white thinking. But the motives for this behavior are different. A narcissist idealizes someone they see as a good source of narcissistic supply. They do not see the source of supply as a person, but will put them on a pedestal as long as they’re providing enough supply. Should the victim stop providing supply (or the narcissist just becomes bored and needs a new source of supply), the narcissist devalues and discards the victim, without mercy or regret.
Most borderlines idealize and devalue others based on their need for acceptance and love, not the need for supply. If they perceive another person as good and kind, and accepting of them, they will tend to idealize the person and sometimes become clingy and needy (a narcissist can be clingy and needy too, but for different reasons). If the borderline feels the other person losing interest or pulling away from them, they may suddenly, without warning, devalue the other person and reject them. They do this not to be mean, but to avoid being rejected themselves. This explains the “I hate you…don’t leave me” or “come closer…go away” behaviors many borderlines show. It’s confusing and contradictory to others, but it helps them to avoid the inevitable rejection they believe is coming to them. Borderlines live in constant fear of being rejected; narcissists live in constant fear being ignored–losing their “drug” of narcissistic supply. While their behaviors may seem similar on the surface, the motives behind them are quite different.
A borderline is not usually deliberately malicious or sadistic. It’s not their intention to hurt others or cause them misery, even though they unintentionally do it all the time because they have so much trouble controlling their impulses. They usually are not even aware how much their unpredictable and contradictory behavior is confusing or hurting others. If a borderline is made aware of what they are doing, they are far more likely to seek therapy than a narcissist, because someone with BPD wants more than anything to be loved and accepted. A narcissist just doesn’t care what you think of them, as long as you are paying attention to them. Of course, there are some low-mid spectrum narcissists who have enough self awareness and hate the fact they can’t feel the more sublime emotions (love, empathy, joy) of a normal person, and those few may actually seek help too.
BPD is maladaptive to the victim.

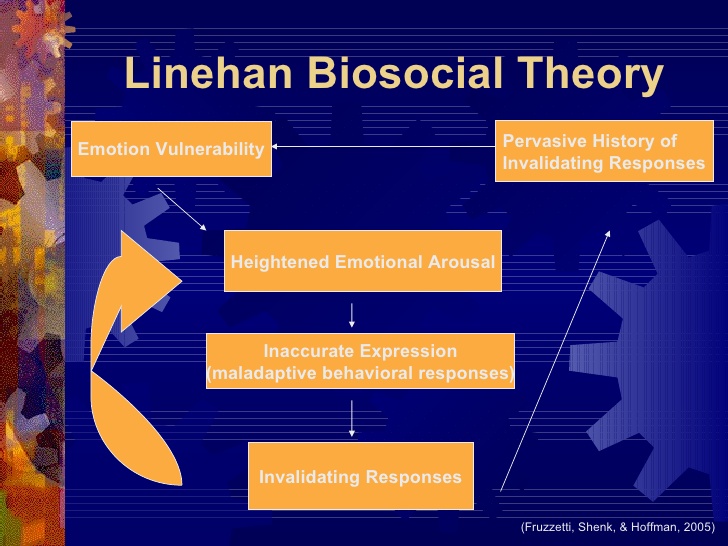
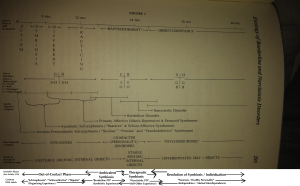
Marsha Linehan’s diagram that shows why BPD doesn’t work well for the sufferer. (click to enlarge)
Borderline personality disorder is ego-dystonic: that is, it isn’t adaptive to the sufferer and their behaviors cause them as much or more misery than it causes others. People with any ego-dystonic disorder or mental illness–depression, anxiety, phobias, certain personality disorders such as Avoidant, Borderline or Dependent–are more likely to seek treatment because they aren’t happy with the way they behave and feel. They don’t necessarily blame others for their own misery, the way a narcissist will do.
Borderlines are also far more likely than narcissists to engage in suicidal ideation or even attempt suicide when they become depressed. They are self-destructive and more dangerous to themslves than others. A narcissist is not as likely to consider or attempt suicide, but if they do, they are more likely to attempt to “take you with them.”
Narcissistic personality disorder is ego-syntonic: that is, it usually is adaptive to the sufferer and in most cases their bad behaviors don’t bother them at all (they don’t care how you feel), they only bother others. This is why narcissists are so unlikely to seek treatment, unless they have lost their sources of supply and are undergoing severe depression (narcissistic crisis). Narcissists are miserable people, but they are far more likely than borderlines to blame others for their own misery.
Both disorders are included under the Cluster B category of personality disorders because both involve a malfunction of emotional regulation. In a narcissist, emotion is strong but is hidden and masked; in a borderline, emotion is strong but cannot be hidden or regulated at all. Both disorders cause others misery, but a narcissist lives a lie; a borderline generally does not.
BPD as a defense mechanism that arises in early childhood.

Both NPD and BPD (and all Cluster B disorders) arise out of childhood from early attachment disorders with caregivers. Both are desperate attempts not to be hurt anymore and have their origins in abuse or neglect as young children. Most narcissists and borderlines were abuse victims as children. Both narcissists and borderlines are incredibly sensitive–so much so, they have constructed almost intractible defense mechanisms to avoid further pain and hurt. Unfortunately for the borderline, their defense mechanism of overreaction to everything is maladaptive and hurts them more than they can hurt anyone else. But due to this, they are far more likely to seek treatment.
Upcoming Post:
Later on, I plan to post an article about Marsha Linehan’s DBT and other therapies for people suffering from Borderline Personality Disorder. (They are similar to the methods used for people with NPD).