I never knew that Antisocial Personality Disorder had different subtypes, but it does make sense that it would. These are Millon’s ten subtypes of ASPD (antisocial personality disorder). Theodore Millon was a psychologist who specialized in personality disorders and subdivided them into various subtypes. (In a future article, I’ll write a post about his Borderline Personality Disorder divisions.)
This was a post I found on Psychforums (in the ASPD forum). I don’t know who wrote it, so I can’t give credit to the original source, only a link to where I found it.
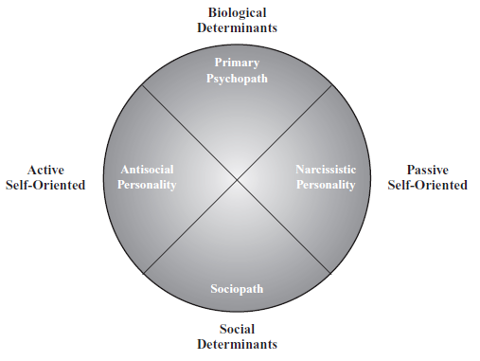
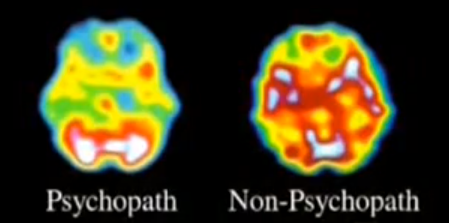
In the post I found, the the term “psychopath” is used, but I think these types more properly describe people with ASPD, most who are sociopaths (an acquired condition due to trauma that may also involve brain dysfunction), not psychopaths (a condition of the brain you are born with that has nothing or little to do with early trauma). There are also pro-social psychopaths (though all psychopaths lack a conscience), and none of these types seem very pro-social to me. So even though many psychopaths may fit these subtypes, I think it’s misleading so I took out the term “psychopath” in the subheads.
Unprincipled
Activities kept near or at the boundaries of the law; stereotyped social roles; con man, charlatan, fast-talking used car salesman.Expansive fantasies and exaggerated sense of self-importance.Willing to take advantage of and humiliate those who leave themselves open to deceit.
May cultivate persuasiveness or charm as a means of getting others to lower their guard, but sees all prosocial behaviour as ultimately self-serving.
Contemptuous of “the system”; working “the system” to avoid punishment seen as just “part of the game“.
Covetous
Sees self as wrongfully deprived of life’s necessities, leading to envy and resentment.
Compensates by taking what he or she is entitled to as a means of revenging wrong and restoring “karmic balance” in life.
Sees self as a victim of external forces, misunderstood by others and by society.
Manipulates others as a meaning of proving own superiority, as well as avenging attributions of worthlessness.
Smug and contemptuous toward victims, who may be viewed as pawns in the larger game.
Prone to ostentatious displays of conspicuous consumption.
Risk-Taking
Chronic underarousal leads to risk-taking as means of “feeling alive”.
Fails to realize the consequences of risk-taking; believes that social rules are unnecessarily confining of own sense of adventure.
Eschews normal desire for safety as evidence of cowardice.
Proves own mettle as a means of proving self-esteem and worthiness to self and others.
Disingenuous
Superficial sociability (or even seductiveness) hides an impulsive, moody and resentful core.
Emotionally labile, prone to excitement-seeking, stimulus-dependant behaviour, lacking in forethought, with a high potential for painful consequences.
Rationalizes and projects blame onto others when attempts to solicit attention go awry.
Spineless
Aggression not intrinsically rewarding; psychopathic acts intended to others that the psychopath is not weak.
Has first-strike mentality; strikes whenever own fearfulness peaks (perhaps in episodes of panic), regardless of objective degree of threat.
Experiences fantasies of vulnerability; sees others as sadistic or exploiting. [my note–I’m not sure what “fantasies of vulnerability” would refer to]
Abrasive
Prefers to be overtly contentious, confrontational, antagonistic rather than indirectly manipulative.
Expects hostility from others, and pre-empts insults with own abrasiveness.
Prefers to escalate arguments; experiences pleasure by frustrating others, making them back down.
Inherently oppositional to any form of emotional control; seeks to break constraints simply because they exist.
Tyrannical
Realizes pleasure through total control of others.
Employs violence instrumentally, to force perceived opponents to cower or submit.
Projects image of power or brutality; supports self-image of power and superiority by inflicting pain and suffering, if not power.
Explosive
Low frustration threshold, resulting in episodes of uncontrollable rage and violent attack.
Episodes may be instantaneous reaction to frustration or perceived insult, and thus may be perceived by others as random and unprovoked.
Malevolent
Hateful, destructive defiance of values of social life.
inherently distrustful, ruthless, cold-blooded, revengeful, punitive.
Malignant
Often isolated, paranoid, with ruminative fantasies of power and revenge.
Sees others as inherently persecutory or treacherous.
Uses hostility as a means of armoring self, forcin adversaries to take issue and withdraw.
http://www.psychforums.com/antisocial-personality/topic95961.html